Causes of Vocal Fold Nodules
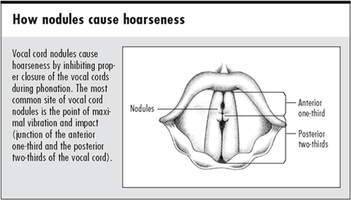
This video provides video stroboscopic images of the larynx and audio recordings of the voice. This individual has been diagnosed with bilateral vocal fold nodules and as you can tell, the quality of her voice has been effected by this organic voice disorder.
According to Buckmire (2013), nodules are most often observed in women aged 20-50 years, but they are also found commonly in children (more frequently in boys than in girls) who are prone to excessive shouting or screaming (n.p.).
Nonneoplastic lesions of the vocal folds are presumed to represent a response to vocal trauma or “phonotrauma”. Buckmire (2013) refereced a study from 1999, that elicited the educated opinions of professionals associated with the voice and those with knowledge of VFN regarding the cause of VFN. A nearly unanimous belief existed amongst all professionals that vocal abuse or misuse was the culprit for causing VFN.
Another study, completed in 2000, attempted to classify vocally traumatic behaviors, such as hard glottal attack, as a cause of vocal fold lesions or nodules. Results indeed confirmed a higher incidence of hard glottal attack in patients presenting with vocal fold nodules.
Buckmire (2013) also referenced a 2005 study featuring pediatric voice patients, hyperfunctional vocal behaviors were found to be associated with the size of the vocal fold nodule(s). Furthermore, parents rated these children as being “outgoing” or “extroverted”, as a reference to the child’s engaging in behaviors classified as vocal abuse and/or misuse, such as excessive screaming.
A study conducted in 1998, referenced by Buckmire (2013), found the prevalence of pharyngeal reflux was significantly higher in patients with VFN.
According to Goldman, Hargrave, Hillman, Holmberg, & Gress (1996), approximately 2/3 of patients presenting with vocal nodules are female (p. 44). The authors conducted a research study in an effort to identify the etiology behind the manifestations of vocal hyperfunction, such as vocal fold nodules (Goldman, Hargrave, Hillman, Holmberg, & Gress, 1996, p. 44). Of particular interest were “psychosocial factors” of psychological stress, anxiety, voice use, and somatic status in females (p. 45).
Goldman, Hargrave, Hillman, Holmberg, & Gress’s (1996) study found the following:
Psychosocial factors long have been associated with the development of hyperfunctional voice disorders such as vocal nodules. However, experimental evidence concerning the role of these factors in the etiology of vocal nodules specifically is sparse. The present study represents a preliminary examination of some psychosocial factors for 3 groups of adult female subjects: 27 with vocal nodules, 17 with hyperfunctionally related voice disorders other than nodules (pathological control), and 33 with no history of voice disorders (normal control). Four psychosocial factors were studied: stress (measured by the Social Readjustment Rating Questionnaire), anxiety (measured by the State-Trait Anxiety Inventory), voice use, and somatic complaints (both measured by our own instruments). Relative to the normal control group, the patients with nodules showed significantly increased scores on all factors except stress. The pathological control group showed significantly increased scores on all factors except voice use. No significant differences were found between the group with nodules and the pathological control group on any factor (p. 44).
According to Buckmire (2013), nodules are most often observed in women aged 20-50 years, but they are also found commonly in children (more frequently in boys than in girls) who are prone to excessive shouting or screaming (n.p.).
Nonneoplastic lesions of the vocal folds are presumed to represent a response to vocal trauma or “phonotrauma”. Buckmire (2013) refereced a study from 1999, that elicited the educated opinions of professionals associated with the voice and those with knowledge of VFN regarding the cause of VFN. A nearly unanimous belief existed amongst all professionals that vocal abuse or misuse was the culprit for causing VFN.
Another study, completed in 2000, attempted to classify vocally traumatic behaviors, such as hard glottal attack, as a cause of vocal fold lesions or nodules. Results indeed confirmed a higher incidence of hard glottal attack in patients presenting with vocal fold nodules.
Buckmire (2013) also referenced a 2005 study featuring pediatric voice patients, hyperfunctional vocal behaviors were found to be associated with the size of the vocal fold nodule(s). Furthermore, parents rated these children as being “outgoing” or “extroverted”, as a reference to the child’s engaging in behaviors classified as vocal abuse and/or misuse, such as excessive screaming.
A study conducted in 1998, referenced by Buckmire (2013), found the prevalence of pharyngeal reflux was significantly higher in patients with VFN.
According to Goldman, Hargrave, Hillman, Holmberg, & Gress (1996), approximately 2/3 of patients presenting with vocal nodules are female (p. 44). The authors conducted a research study in an effort to identify the etiology behind the manifestations of vocal hyperfunction, such as vocal fold nodules (Goldman, Hargrave, Hillman, Holmberg, & Gress, 1996, p. 44). Of particular interest were “psychosocial factors” of psychological stress, anxiety, voice use, and somatic status in females (p. 45).
Goldman, Hargrave, Hillman, Holmberg, & Gress’s (1996) study found the following:
Psychosocial factors long have been associated with the development of hyperfunctional voice disorders such as vocal nodules. However, experimental evidence concerning the role of these factors in the etiology of vocal nodules specifically is sparse. The present study represents a preliminary examination of some psychosocial factors for 3 groups of adult female subjects: 27 with vocal nodules, 17 with hyperfunctionally related voice disorders other than nodules (pathological control), and 33 with no history of voice disorders (normal control). Four psychosocial factors were studied: stress (measured by the Social Readjustment Rating Questionnaire), anxiety (measured by the State-Trait Anxiety Inventory), voice use, and somatic complaints (both measured by our own instruments). Relative to the normal control group, the patients with nodules showed significantly increased scores on all factors except stress. The pathological control group showed significantly increased scores on all factors except voice use. No significant differences were found between the group with nodules and the pathological control group on any factor (p. 44).
Vocal Abuse and Misuse
According
to Boone, McFarlane, Von Berg, & Zraick (2010), “Vocal abuse comprises
various behaviors and events that have some kind of deleterious effect on the
larynx and the voice, such as:
Vocal misuse means improper use of voice, such as:
Vocal abuse and misuse behaviors can create physical changes such as nodules, polyps, and contact ulcers related to vocal hyperfunction (p. 203).
- Yelling and screaming
- Speaking against a background
of loud noise
- Coughing and excessive throat
clearing
- Smoking
- Excessive talking or singing
- Excessive talking or singing
while having an allergy or upper respiratory infection
- Excessive crying or laughing
- Weight lifting with effortful
“grunts”
Vocal misuse means improper use of voice, such as:
- Speaking with hard glottal
attack
- Singing excessively at the
lower or upper end of one’s range
- Increasing vocal loudness by
squeezing out the voice at the level of the larynx
- Speaking at excessive intensity
levels
- Cheerleading
- Speaking over time at an
inappropriate pitch level
- Speaking or singing (such as a
prolonged show rehearsal) for excessively long periods of time" (p. 203).
Vocal abuse and misuse behaviors can create physical changes such as nodules, polyps, and contact ulcers related to vocal hyperfunction (p. 203).
Are Vocal Fold Nodules Cancerous?
Vocal
fold nodules are considered benign vocal lesions, indicating VFN as
non-cancerous growths of abnormal tissue on the vocal folds. A clinical diagnosis of nodules does not rule
out a malignancy (cancer) unless the lesion resolves without treatment or is
biopsied and found to be pathologically benign.
Suspicious lesions, an enlarging lesion, and lesions having failed
medical, behavioral, and speech therapy are all indications for biopsy and
possible removal as these are possible signs for malignancy.
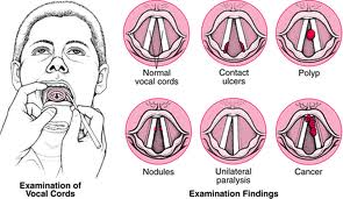

Bilateral Vocal Fold Nodules

Laryngeal Cancer
Reflux
According to Kunh et. al, (1998), “Gastroesophageal reflux has been
implicated in the pathogenesis of vocal cord nodules. However, a
cause-and-effect relationship has not been established”.
Kunh et. al, (1998) conducted a study to determine the frequency of pharyngeal acid reflux events in clients with vocal nodules. Participants included eleven patients with vocal nodules and eleven healthy individuals. All patients underwent barium esophagram and ambulatory 24-hour simultaneous three-site pharyngoesophageal pH monitoring. In the ambulatory pH monitoring studies, pH was recorded from the manometrically determined sites of pharynx (2 cm above upper esophageal sphincter), proximal esophagus (10 cm distal to pharyngeal site), and distal esophagus (5 cm above the lower esophageal sphincter). Pharyngeal acid reflux event was deemed acceptable if all three sites recorded a decrease in pH below 4, which was not related to meal or drinking. Kunh et. al (1998) found that pharyngeal acid reflux events occurred in seven of 11 patients with vocal nodules and two of 11 controls. For both groups, pharyngeal acid reflux events occurred in the upright position and not associated with belching or coughing (Kunh et. al, 1998). Kunh and colleagues (1998) concluded that “prevalence of pharyngeal acid reflux events are significantly higher in patients with vocal nodules compared with normal controls and suggests a contributory role for gastroesophagopharyngeal acid reflux in the pathogenesis of some vocal cord nodules.”
Kunh et. al, (1998) conducted a study to determine the frequency of pharyngeal acid reflux events in clients with vocal nodules. Participants included eleven patients with vocal nodules and eleven healthy individuals. All patients underwent barium esophagram and ambulatory 24-hour simultaneous three-site pharyngoesophageal pH monitoring. In the ambulatory pH monitoring studies, pH was recorded from the manometrically determined sites of pharynx (2 cm above upper esophageal sphincter), proximal esophagus (10 cm distal to pharyngeal site), and distal esophagus (5 cm above the lower esophageal sphincter). Pharyngeal acid reflux event was deemed acceptable if all three sites recorded a decrease in pH below 4, which was not related to meal or drinking. Kunh et. al (1998) found that pharyngeal acid reflux events occurred in seven of 11 patients with vocal nodules and two of 11 controls. For both groups, pharyngeal acid reflux events occurred in the upright position and not associated with belching or coughing (Kunh et. al, 1998). Kunh and colleagues (1998) concluded that “prevalence of pharyngeal acid reflux events are significantly higher in patients with vocal nodules compared with normal controls and suggests a contributory role for gastroesophagopharyngeal acid reflux in the pathogenesis of some vocal cord nodules.”
Nodules in specific populations
Vocal fold nodules are most commonly found in women (ages 20-50) and male children (prone to excessive shouting and screaming). However, specific populations experience VFN in abundance, such as teachers, cheerleaders, clergy members, singers, and any professionals relying on their voice in order to perform the duties of their corresponding job.

Symptoms of Vocal Fold Nodules

According
to the American Academy of Otolaryngology – Head and Neck Surgery, vocal fold
nodules (VFN) may also be referred to as “vocal cord nodules”, “singer’s nodes”,
“screamer’s nodes”, or “calluses of the vocal fold”.
Often, the first signs of VFN include persistent hoarseness and/or a change in voice quality. Other symptoms may include the following:
Often, the first signs of VFN include persistent hoarseness and/or a change in voice quality. Other symptoms may include the following:
- Vocal fatigue
- Unreliable voice
- Delayed voice initiation
- Low, gravelly voice
- Low pitch
- Voice breaks in first passages of
sentences
- Airy or breathy voice
- Inability to sing in high, soft voice
- Increased effort to speak or sing
- Hoarse and rough voice quality
- Frequent throat clearing
- Extra force needed for voice
- Voice "hard to find"
The severity of symptoms may increase or decrease, but will continue to persist and will not go away without intervention.

This link http://www.uchospitals.edu/online-library/content=P00475, will take you directly to a table that explains how to distinguish the difference between the different types of laryngeal disorders.
This in-service provides an introductory education to individuals who are interested in obtaining information regarding the pathology, assessment and treatment of vocal nodules.
