Dr. James Thomas explains how vocal fold nodules occur and what they look like.
What are Vocal Fold Nodules?
Vocal nodules are the most common, benign (non-cancerous) lesions of the vocal folds. This holds true for both adults and children. According to Boone, McFarlane, Von Berg, and Zraick (2010), vocal nodules are "Bilateral, midmembraneous, vocal fold lesions of the basement membrane zone and the superficial layer of the lamina propria" (pg. 123). They are caused by continuous abuse of the larynx and misuse of the voice, which may also be called "vocal hyperfunction".
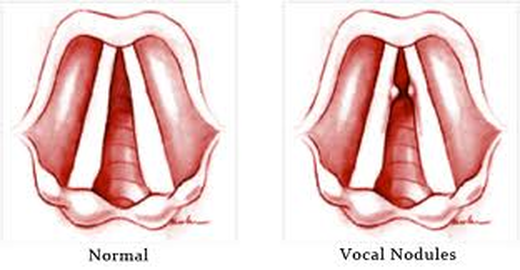
(LEFT) The normal anatomy of the Vocal
Folds.
(RIGHT) The appearance of Vocal Nodules on the Vocal Folds.
(RIGHT) The appearance of Vocal Nodules on the Vocal Folds.
What are the symptoms of Vocal Fold Nodules?
Often, the
first signs of vocal fold nodules include persistent hoarseness and/or a change in voice
quality. Other symptoms may include the
following:
- Vocal fatigue
- Unreliable voice
- Delayed voice initiation
- Low, gravelly voice
- Low pitch
- Voice breaks in first passages of
sentences
- Airy or breathy voice
- Inability to sing in high, soft voice
- Increased effort to speak or sing
- Hoarse and rough voice quality
- Frequent throat clearing
- Extra force needed for voice
- Voice "hard to find"
What do Vocal Fold Nodules look like?
Vocal fold nodules are typically bilateral, whitish protuberances on the glottal margin of each true vocal fold, located at the anterior- middle third junction. The anterior-middle third junction is known as the "classic description" of location for vocal fold nodules. Vocal fold nodules can vary considerably in size, number, and location. For example, nodules may range from one to four in number, known as "quad nodules".
Course of Development for vocal fold nodules is as follows:
The nodule(s) begin as soft and pliable. As phonotrauma continues, the soft, pliable nodule becomes increasingly fibrotic and may either become much more focused, smaller, and harder OR it may increase in size.
Course of Development for vocal fold nodules is as follows:
The nodule(s) begin as soft and pliable. As phonotrauma continues, the soft, pliable nodule becomes increasingly fibrotic and may either become much more focused, smaller, and harder OR it may increase in size.
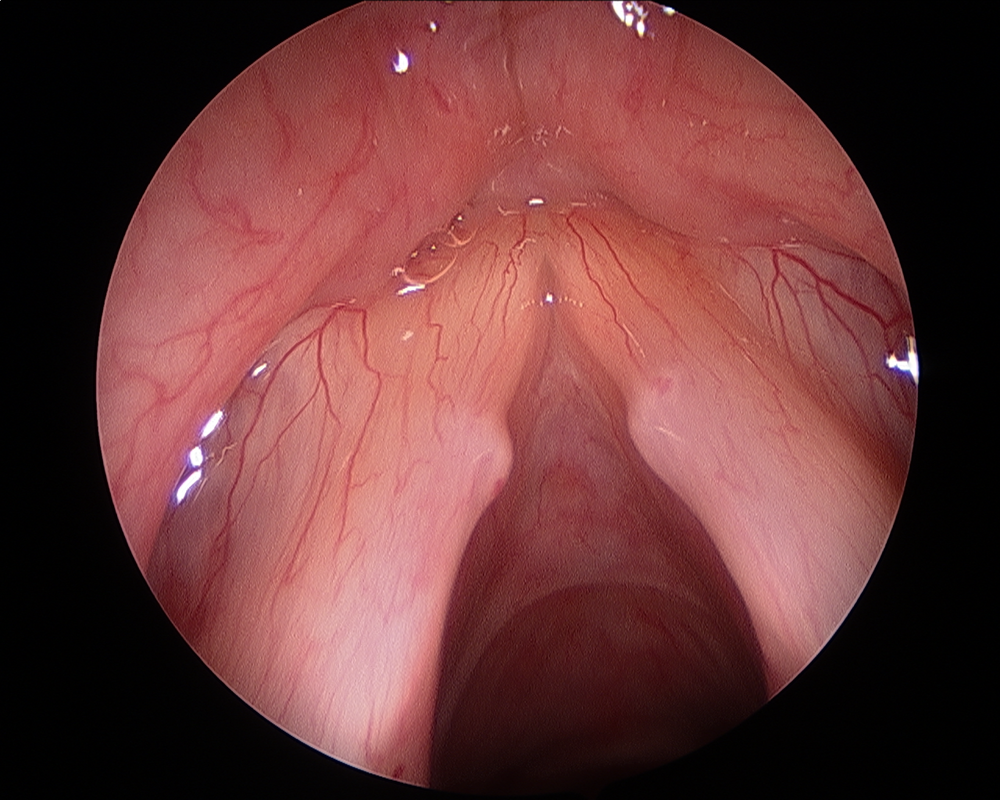
Bilateral Vocal Fold Nodules
How are Vocal Fold Nodules treated?

According to ASHA (2014), vocal nodules can be treated
surgically, medically, and/or behaviorally. Surgical treatment involves the
surgical removal of the nodules from the vocal folds. This approach is typically
only used when the nodules are very large or if they have been present for a
long period of time. Surgical removal of vocal nodules is rare in children
(ASHA, 2014). Medical intervention of
vocal nodules involves treating the medical conditions that cause the nodule.
Examples of medical problems that can cause vocal nodules include
gastroesophageal reflux disease (GERD), allergies, and thyroid conditions ASHA,
2014).
The behavioral treatment for vocal nodules involves voice therapy from an SLP. The voice therapy will involve a vocal hygiene program, which will work to reduce/eliminate vocal misuse and abuse behaviors. Voice therapy will also involve direct voice treatment to improve pitch, loudness, quality, and respiratory support. Stress reduction and relaxation techniques will also be emphasized in vocal therapy for the treatment of vocal nodules (ASHA, 2014).
The behavioral treatment for vocal nodules involves voice therapy from an SLP. The voice therapy will involve a vocal hygiene program, which will work to reduce/eliminate vocal misuse and abuse behaviors. Voice therapy will also involve direct voice treatment to improve pitch, loudness, quality, and respiratory support. Stress reduction and relaxation techniques will also be emphasized in vocal therapy for the treatment of vocal nodules (ASHA, 2014).
Video explaining vocal nodules and how the voice works.
Vocal Fold Nodules and the voice
As the bilateral
nodules approximate one another on phonation, there is usually an open glottal
chink anterior and posterior to the nodule contact point, which results in a
glottal hourglass figure. This open
glottal chink (produced by the nodules coming together in exact opposition of
one another) results in a lack of complete vocal fold adduction.
(Boone, McFarlane, Von Berg, & Zraick, 2010, p. 123)
The fault approximation of the vocal folds creates air wastage and breathiness in the client's voice.
Furthermore, vocal fold nodules create extra mass on the vocal folds, which creates a lower pitch and increased aperiodocity.
(Boone, McFarlane, Von Berg, & Zraick, 2010, p. 123)
The fault approximation of the vocal folds creates air wastage and breathiness in the client's voice.
Furthermore, vocal fold nodules create extra mass on the vocal folds, which creates a lower pitch and increased aperiodocity.
- Pitch: the rate of vibration of the vocal folds ( Sound changes as rate of vibration changes).
- Increase Aperiodocity = hoarseness.
The experience of the client with
Vocal Fold Nodules
- Vocal fold nodules are more common in young boys in
the childhood population.
- In the adolescent and adult populations, females
have a higher prevalence of nodules.
- Clients may complain of the constant need to clear
his or her throat.
- Excessive throat clearing is identified as a form of vocal abuse.
- Excessive throat clearing is identified as a form of vocal abuse.
- The client may experience excessive mucous on the
folds.
- The client’s voice may deteriorate with continuous
voicing.
- For example: The client may begin the day with a “good” or “normal” voice
that continues to deteriorate or become “dysphonic” with continuous use.
- For example: The client may begin the day with a “good” or “normal” voice
that continues to deteriorate or become “dysphonic” with continuous use.
- A large population of clients experiencing VFN
include cheerleaders, teachers, clergy members, singers.
